Endometriosis: Symptoms, Causes and Treatment Options Explained
INTRO
Endometriosis affects roughly 1 in 10 women of reproductive age, yet it takes an average of several years for most women to receive a correct diagnosis. Part of the problem is that its symptoms are frequently dismissed as “just bad periods” — by doctors, by family, and sometimes by women themselves who have been told their whole lives that period pain is simply something to push through. This delay in diagnosis can mean years of unnecessary suffering and, in some cases, missed opportunities for earlier treatment. In this article we’ll break down exactly what endometriosis is, the full range of symptoms to watch for, why it is so often missed or misdiagnosed, how doctors confirm a diagnosis, and what treatment options exist depending on your goals and symptom severity.
What Is Endometriosis?
Endometriosis occurs when tissue similar to the lining of the uterus — called the endometrium — grows outside the uterus, most commonly on the ovaries, fallopian tubes, the outer surface of the uterus, and the lining of the pelvic cavity. In rarer cases it can be found in other areas of the body entirely.
Each month, this displaced tissue responds to the same hormonal signals that drive your menstrual cycle, thickening and attempting to shed just like the normal uterine lining does. The problem is that this tissue has no way to leave the body the way a period does. Instead, it becomes trapped, leading to inflammation, irritation of surrounding tissue, and over time the formation of scar tissue and adhesions that can bind pelvic organs together.
According to the Office on Women’s Health, endometriosis affects roughly 11% of American women between ages 15 and 44, and diagnosis is frequently delayed by several years due to the overlap between its symptoms and other common conditions.
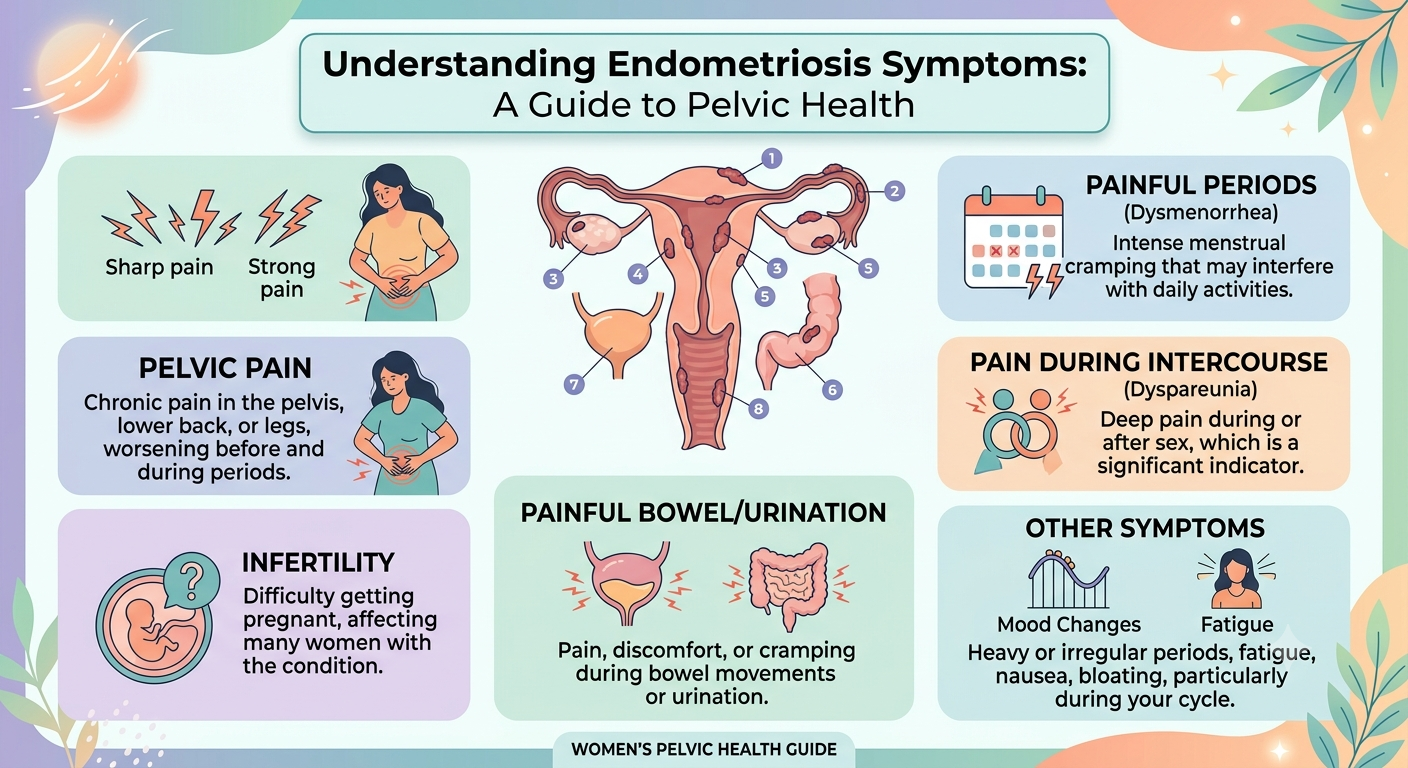
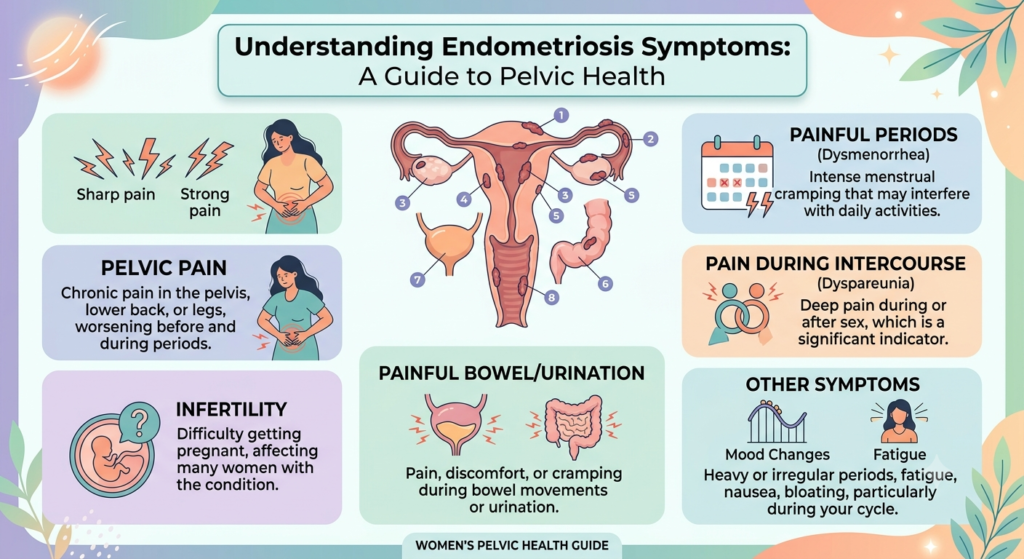
Common Symptoms of Endometriosis
Endometriosis symptoms vary considerably between women — some experience severe pain with relatively little tissue found during surgery, while others have extensive tissue with minimal symptoms. That said, several patterns are widely recognized.
Severe Period Pain
This is the hallmark symptom — pain that doesn’t respond well to typical over-the-counter pain relief like ibuprofen, that may begin before your period starts, and that can be severe enough to interfere with work, school, or daily activities. This is different from the mild to moderate cramping many women experience normally.
Pain During or After Intercourse
Often described as a deep ache rather than surface discomfort, this pain can occur during intercourse itself or persist for hours afterward, and is one of the more commonly reported but less openly discussed symptoms.
Heavy or Irregular Bleeding
Many women with endometriosis experience heavier than average periods, longer periods, or spotting between cycles. Track your patterns over several months using our Free Period Tracker so you have concrete data to discuss with your doctor rather than relying on memory.
Chronic Pelvic Pain
Unlike pain that is limited strictly to your period, many women with endometriosis experience a persistent, dull pelvic ache that continues throughout the month and may worsen around ovulation or before menstruation.
Digestive Symptoms
Bloating, diarrhea, constipation, and nausea are common, particularly around the time of your period. This overlap with digestive conditions is one of the major reasons endometriosis is so frequently mistaken for IBS.
Fertility Challenges
Endometriosis is found in a significant proportion of women experiencing difficulty conceiving, though it’s important to note that many women with endometriosis do conceive without medical intervention. The relationship between endometriosis and fertility is complex and depends heavily on the location and extent of the tissue.
Fatigue
Chronic pain and inflammation can contribute to persistent fatigue that doesn’t improve with rest, a symptom that is often overlooked but frequently reported by women living with the condition.
Why Is Endometriosis So Often Missed?
Several factors contribute to the lengthy diagnostic delay that characterizes endometriosis for most women.
Its symptoms overlap heavily with other conditions — irritable bowel syndrome, ovarian cysts, and pelvic inflammatory disease can all present similarly, leading to misdiagnosis.
There is also a persistent cultural normalization of period pain. Many women are told from adolescence that significant pain during periods is simply part of being a woman, which discourages them from seeking further evaluation when something is genuinely abnormal.
Definitive diagnosis traditionally requires a surgical procedure, which means many doctors are hesitant to pursue it until symptoms become severe or fertility becomes a concern, further extending the time to diagnosis.
The key takeaway here is this: severe pain that disrupts daily life is never something to simply accept as normal, regardless of what you may have been told previously.
How Is Endometriosis Diagnosed?
Diagnosis typically follows a staged process.
Step 1 — Symptom history and pelvic exam. Your doctor will ask detailed questions about your pain patterns, cycle, and any other symptoms, followed by a physical pelvic exam to check for tenderness or abnormalities.
Step 2 — Imaging. Ultrasound, and in some cases MRI, can identify larger endometriomas (cysts caused by endometriosis on the ovaries) but cannot detect smaller areas of tissue.
Step 3 — Laparoscopy. A definitive diagnosis typically requires laparoscopy, a minimally invasive surgical procedure performed under general anesthesia that allows a surgeon to directly visualize — and often simultaneously treat — endometrial tissue using small incisions and a camera.
Treatment Options for Endometriosis
Treatment is highly individualized based on symptom severity, whether fertility is a current priority, and how the condition is affecting quality of life.
Pain Management
NSAIDs like ibuprofen are often a first step, though for many women with endometriosis these provide only partial relief, which is itself a signal worth mentioning to your doctor.
Hormonal Therapy
Hormonal birth control, including the combined pill, hormonal IUD, or other progestin-based options, can suppress the menstrual cycle and slow the growth of endometrial tissue, often providing significant symptom relief for many women.
GnRH Agonists
These medications induce a temporary menopause-like state to shrink endometrial tissue and are typically used for a limited duration due to their effect on bone density with longer-term use.
Surgery
Laparoscopic excision surgery can remove endometrial tissue and adhesions, often improving both pain and fertility outcomes. This is usually considered when other treatments haven’t provided adequate relief or when fertility is a priority.
If fertility is a concern, discuss treatment timing carefully with a reproductive specialist, and track your cycle with our Free Ovulation Calculator in the meantime to better understand your own patterns.
Living With Endometriosis Day to Day
Beyond medical treatment, many women find that certain lifestyle adjustments help manage symptoms alongside their treatment plan. Heat therapy, gentle exercise, anti-inflammatory dietary changes, and stress management techniques are commonly reported as helpful, though none of these replace medical care for a condition of this nature.
Connecting with others who understand the condition — whether through a support group or simply trusted friends and family — can also make a meaningful difference in how manageable the day-to-day experience feels.
Frequently Asked Questions
Can endometriosis go away on its own?
No, it typically requires ongoing management; it doesn’t resolve without treatment, though symptoms can fluctuate in severity over time and sometimes improve temporarily during pregnancy or with certain hormonal treatments.
Does endometriosis always cause infertility?
No — many women with endometriosis conceive naturally without any intervention, though the condition can reduce fertility in some cases depending on its severity and location.
Is endometriosis the same as fibroids?
No, they are different conditions. Fibroids are noncancerous growths within the uterine wall itself, while endometriosis involves uterine-like tissue growing outside the uterus. Both can cause heavy bleeding and pelvic pain, which sometimes leads to confusion between the two.
Can diet help endometriosis symptoms?
Some women find anti-inflammatory diets — emphasizing vegetables, omega-3s, and reducing processed foods — help manage symptoms alongside medical treatment, though this isn’t a substitute for proper diagnosis and care.
At what age does endometriosis typically start?
It can begin shortly after a person’s first period, though it is often not diagnosed until years later. Symptoms can persist or worsen through the reproductive years and typically improve after menopause.
The Bottom Line
If your period pain is severe, worsening over time, or disrupting your daily life in any meaningful way, it is absolutely worth raising endometriosis with your doctor specifically rather than assuming it’s simply something to endure. Track your symptoms in detail with our Free Period Tracker to bring concrete, dated information to your appointment — this kind of documentation often makes a real difference in how quickly you’re taken seriously and properly evaluated.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult your doctor or OB-GYN for personal health decisions. Read our full Medical Disclaimer.