Luteal Phase Defect: Symptoms, Causes and What to Do
INTRO
If you have been trying to conceive without success, or if you have experienced early miscarriages, you may have come across the term luteal phase defect. It is one of those conditions that does not get talked about nearly enough — yet it affects more women than most people realize and can have a significant impact on fertility. The good news is that luteal phase defect is diagnosable, treatable, and very manageable once you know what you are dealing with. In this article we are going to cover exactly what the luteal phase is, what a defect means, how to recognize the symptoms, what causes it, and what your options are if you think it might be affecting your cycle.
What Is the Luteal Phase?
To understand luteal phase defect you first need to understand what the luteal phase actually is and what role it plays in your cycle.
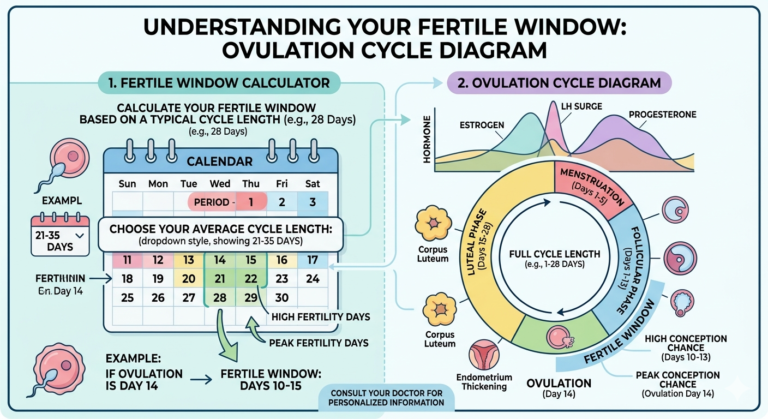
Your menstrual cycle is divided into two main halves. The first half — called the follicular phase — starts on day 1 of your period and ends at ovulation. During this phase your body prepares a follicle to release an egg.
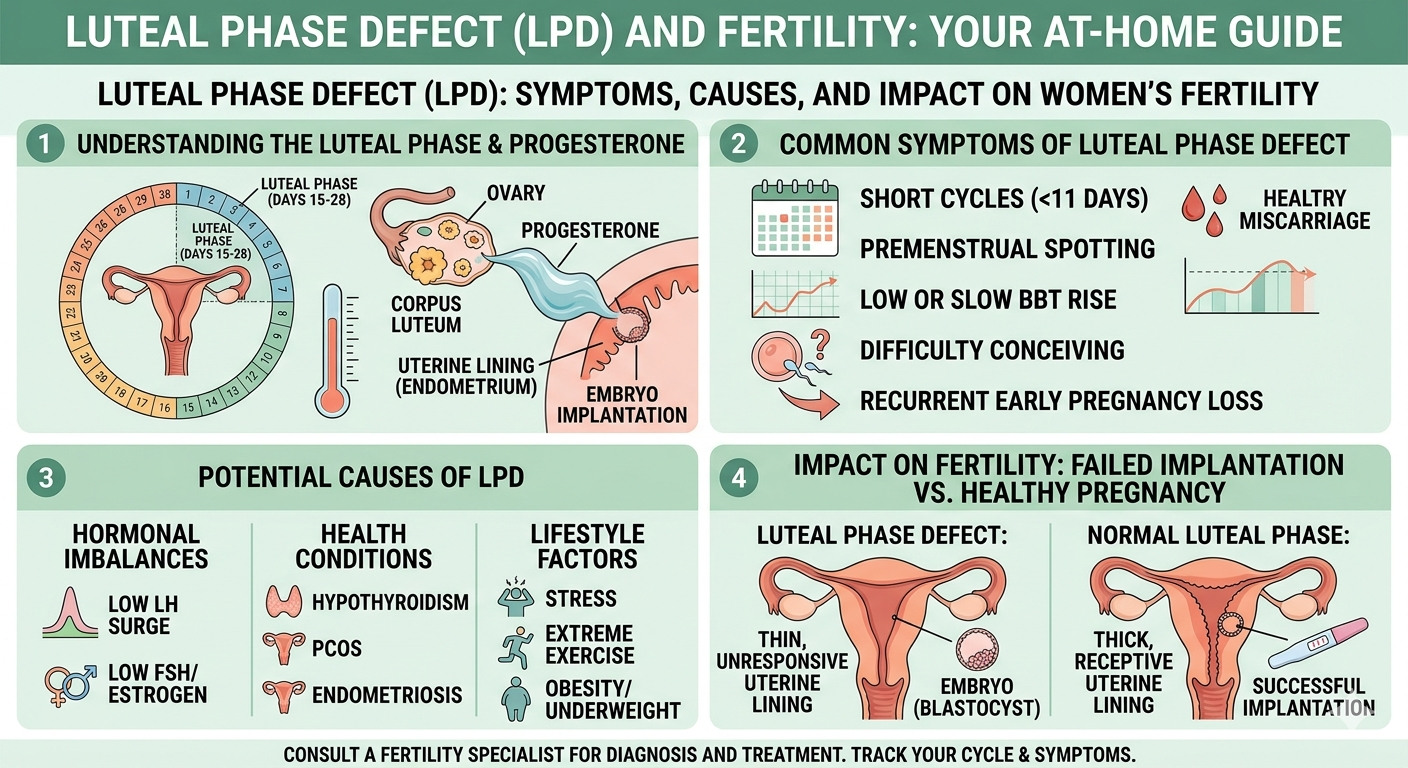
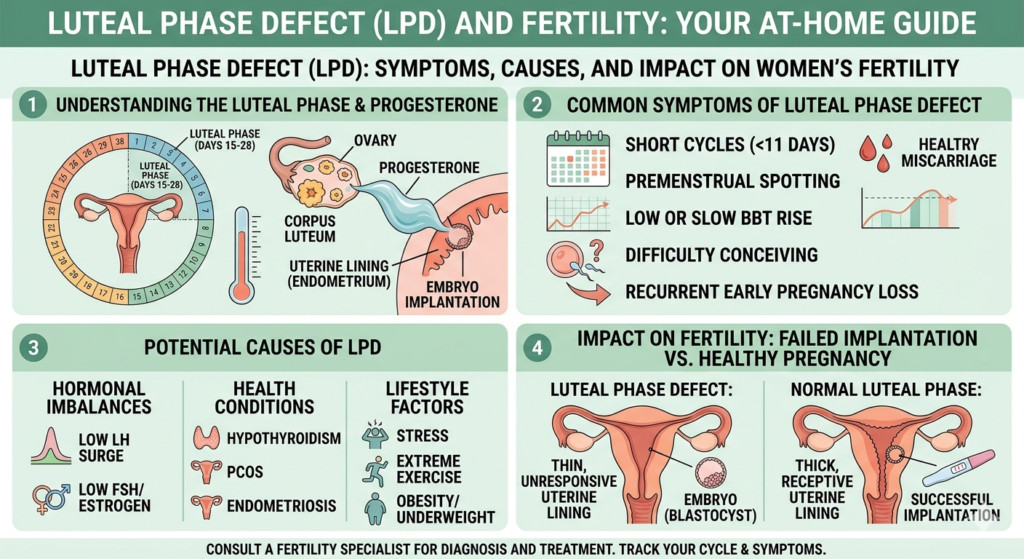
The second half is the luteal phase. It begins immediately after ovulation and ends when your next period starts. During the luteal phase the empty follicle that released your egg transforms into a structure called the corpus luteum, which produces progesterone.
Progesterone is essential. It thickens the uterine lining to prepare it for a fertilized egg to implant. It also keeps the lining stable and intact long enough for a pregnancy to establish itself. Without sufficient progesterone the uterine lining breaks down too early — and either implantation cannot occur or a very early pregnancy is lost before it even registers on a test.
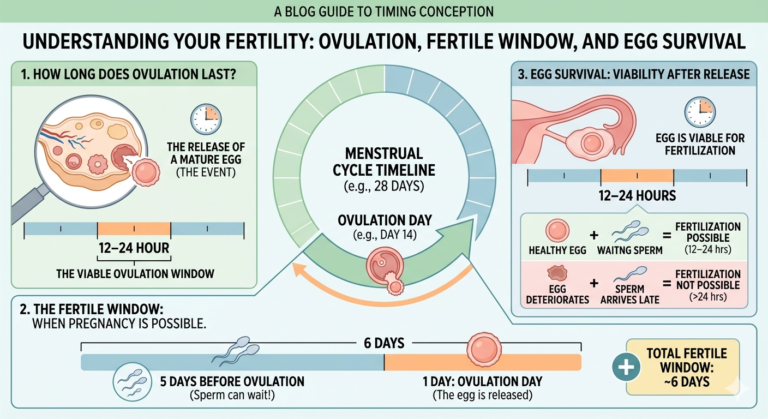
A normal luteal phase lasts between 12 and 16 days. Most women have a luteal phase of around 14 days. Use our Free Ovulation Calculator to estimate your own luteal phase length based on your cycle data.
What Is Luteal Phase Defect?
Luteal phase defect — also called luteal phase insufficiency or LPD — is a condition in which either the luteal phase is too short or the corpus luteum does not produce enough progesterone to adequately support the uterine lining.
There are two ways luteal phase defect can present:
Short luteal phase: The luteal phase lasts fewer than 10 days. When this happens the uterine lining sheds too soon after ovulation — meaning a fertilized egg does not have enough time to implant before the next period begins.
Insufficient progesterone: The luteal phase may be a normal length but progesterone levels are too low to adequately prepare or maintain the uterine lining. This can prevent implantation or lead to very early pregnancy loss.
It is worth noting that luteal phase defect is a somewhat debated diagnosis in the medical community. According to the American Society for Reproductive Medicine, there is no single universally agreed-upon diagnostic standard, which means it can sometimes be underdiagnosed or overlooked.
Luteal Phase Defect Symptoms
Luteal phase defect does not always cause obvious symptoms — which is part of why it can be missed. However there are several signs that may indicate your luteal phase is too short or your progesterone is insufficient.
Short Cycle or Early Period
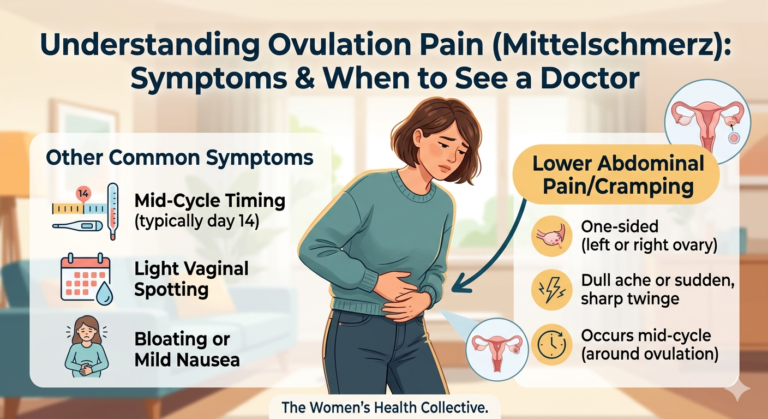
One of the most common signs of luteal phase defect is a noticeably short menstrual cycle — typically fewer than 24 to 25 days in total. If your period seems to arrive too soon after ovulation, or if you notice spotting beginning just 7 to 9 days after you ovulate, your luteal phase may be shorter than it should be.
Spotting Before Your Period
Light spotting or brown discharge in the days before your period officially begins — known as premenstrual spotting — is one of the most frequently reported symptoms of luteal phase defect. This happens because progesterone levels drop too early, causing the uterine lining to begin shedding before your period is due.
If you consistently notice 2 or more days of spotting before your full flow begins it is worth mentioning to your doctor.
Difficulty Getting Pregnant
Because luteal phase defect interferes with implantation, one of its most significant consequences is difficulty conceiving despite regular ovulation and intercourse during the fertile window. If you have been trying to conceive for 6 months or more without success, luteal phase defect is one of several possible factors worth investigating.
Track your cycle carefully using our Free Ovulation Calculator and our Free Period Tracker to gather data that can help your doctor make a more informed assessment.
Recurrent Early Miscarriage
Luteal phase defect is associated with recurrent early pregnancy loss — miscarriages that happen very early in the first trimester, sometimes before a woman even knows she was pregnant. If you have experienced two or more early miscarriages, discussing luteal phase defect with your doctor or a reproductive endocrinologist is an important step.
Mild PMS Symptoms
Some women with luteal phase defect report milder than usual PMS symptoms — particularly less breast tenderness in the second half of their cycle. This can be a sign that progesterone levels are lower than they should be, since progesterone is responsible for many typical premenstrual symptoms.
What Causes Luteal Phase Defect?
Luteal phase defect can have several underlying causes. Identifying the cause is an important part of finding the right treatment.
Hormonal Imbalances
The most common cause is an imbalance in the hormones that regulate the luteal phase — particularly low levels of follicle-stimulating hormone (FSH) or LH during the follicular phase, which results in poor corpus luteum development and insufficient progesterone production after ovulation.
Thyroid Disorders
Both hypothyroidism (underactive thyroid) and hyperthyroidism (overactive thyroid) can disrupt the hormonal balance required for a healthy luteal phase. The thyroid plays a key role in regulating reproductive hormones, and even mildly abnormal thyroid function can affect the luteal phase. A simple blood test can check your thyroid levels.
Hyperprolactinemia
Elevated prolactin levels — a condition called hyperprolactinemia — can interfere with progesterone production and shorten the luteal phase. Prolactin is the hormone responsible for milk production, and abnormally high levels outside of breastfeeding can disrupt the normal hormonal cycle.
Polycystic Ovary Syndrome (PCOS)
PCOS is one of the most common hormonal disorders affecting women of reproductive age and can contribute to luteal phase defect by disrupting ovulation quality and the hormonal signals that follow it.
High Stress Levels
Chronic stress elevates cortisol, which can suppress progesterone production and shorten the luteal phase. This is one of the reasons that significant life stress — a new job, a move, a loss — can suddenly affect your cycle in ways that were not previously an issue.
Extreme Exercise or Low Body Weight
Very high levels of exercise or significantly low body weight can suppress reproductive hormone production, affecting both ovulation and the quality of the luteal phase. Female athletes and women with very low body fat percentages are more likely to experience luteal phase issues.
Age
As women approach perimenopause hormonal fluctuations become more pronounced and the luteal phase can become shorter and more irregular. This is a natural part of the reproductive aging process.
How Is Luteal Phase Defect Diagnosed?
Because there is no single agreed-upon diagnostic test, luteal phase defect is typically diagnosed through a combination of methods.
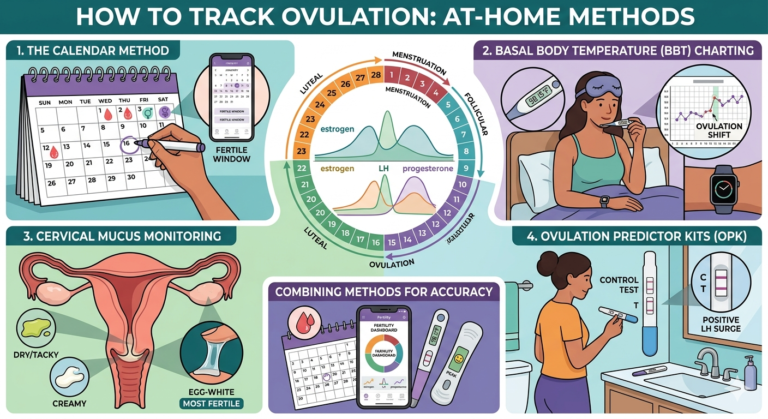
BBT Charting
Charting your basal body temperature over several months can reveal a short luteal phase. If the elevated temperature phase — the post-ovulation rise — consistently lasts fewer than 10 to 12 days this is a strong indicator of a short luteal phase worth discussing with your doctor.
Progesterone Blood Test
A blood test measuring progesterone levels on day 21 of your cycle (or 7 days after ovulation if your cycle is irregular) is one of the most direct ways to assess luteal phase function. Progesterone levels above 10 ng/mL are generally considered indicative of adequate ovulation. Levels below this threshold may suggest luteal phase defect.
Endometrial Biopsy
In some cases a doctor may recommend an endometrial biopsy — a small sample of the uterine lining — to assess whether it is developing appropriately in response to progesterone. This is less commonly used today than it once was but may still be recommended in complex cases.
Ultrasound Monitoring
Transvaginal ultrasound can be used to monitor follicle development and confirm ovulation is occurring normally, which provides useful context for evaluating the luteal phase.
Treatment Options for Luteal Phase Defect
The good news about luteal phase defect is that there are effective treatment options available — many of them straightforward.
Progesterone Supplementation
The most direct treatment is progesterone supplementation, typically given as vaginal suppositories, oral capsules, or injections starting after ovulation is confirmed. This supports the uterine lining during the implantation window and early pregnancy. Progesterone supplementation is commonly used in fertility treatments and has a strong safety record.
Clomiphene Citrate
Clomid (clomiphene citrate) is a medication that stimulates stronger ovulation by prompting the pituitary gland to release more FSH and LH. A stronger ovulation often results in better corpus luteum function and higher progesterone production afterward. Your doctor may prescribe this if your luteal phase defect appears to stem from insufficient follicle development.
Treating the Underlying Cause
If your luteal phase defect is caused by a thyroid disorder, elevated prolactin, or PCOS, treating the underlying condition often resolves the luteal phase issue. This is why thorough blood work and hormone testing is an important first step before jumping straight to progesterone supplementation.
Lifestyle Changes
If high stress, extreme exercise, or low body weight is contributing to your luteal phase defect, addressing these factors can make a meaningful difference. Stress reduction techniques, moderate rather than intense exercise, and achieving a healthy weight for your body can all support better hormonal balance and a healthier luteal phase.
Nutritional Support
Some research suggests that certain nutrients support progesterone production and luteal phase health. These include vitamin B6, vitamin C, zinc, and magnesium. A prenatal vitamin covering these bases is a reasonable starting point — discuss specific supplementation with your doctor before starting anything new.
Tracking Your Luteal Phase at Home
One of the most empowering things you can do if you suspect luteal phase defect is to start tracking your cycle in detail right now. The more data you have when you see your doctor the better.
Here is what to track:
Ovulation date: Use OPK tests and cervical mucus monitoring to identify when you ovulate each cycle. Our Free Ovulation Calculator can give you an estimated ovulation date to start from.
BBT: Chart your basal body temperature daily to identify when your post-ovulation temperature rise begins and how long it lasts.
Cycle length and period start date: Log each period start date carefully using our Free Period Tracker to identify patterns across multiple cycles.
Premenstrual spotting: Note any days of light spotting before your period officially begins — this is important information for your doctor.
After 2 to 3 months of detailed tracking you will have concrete data to bring to your appointment rather than a vague sense that something feels off.
When to See a Doctor
Make an appointment with your doctor or OB-GYN if any of the following apply to you:
You have been trying to conceive for 6 months or longer without success and you are under 35. If you are 35 or older the recommendation is to seek evaluation after 3 months of trying.
You have experienced two or more early miscarriages.
Your BBT charts consistently show a luteal phase shorter than 10 days.
You experience consistent premenstrual spotting beginning more than 2 days before your period.
Your cycles are consistently shorter than 24 days.
A reproductive endocrinologist — a fertility specialist — is the most appropriate specialist if you have been trying to conceive and suspect a hormonal issue. Your OB-GYN can provide a referral.
Frequently Asked Questions
How short is too short for a luteal phase?
A luteal phase shorter than 10 days is generally considered too short to support successful implantation. A luteal phase of 10 to 16 days is considered normal. Most women have a luteal phase of around 12 to 14 days.
Can luteal phase defect cause a missed period?
Luteal phase defect typically causes early periods rather than missed periods — because the lining breaks down too soon. However in some cases hormonal disruption can cause irregular cycles including delayed or missed periods.
Can I get pregnant with luteal phase defect?
Yes — many women with luteal phase defect conceive, particularly with treatment. Progesterone supplementation is highly effective at supporting the uterine lining during the implantation window. Early diagnosis and treatment gives you the best chance of a successful pregnancy.
Is luteal phase defect the same as low progesterone?
They are closely related but not identical. Low progesterone is the most common cause of luteal phase defect, but a luteal phase can also be defective if it is simply too short — even if progesterone levels are within normal range. A thorough hormonal evaluation looks at both the length of the luteal phase and the progesterone levels within it.
Can stress cause luteal phase defect?
Yes. Chronic stress raises cortisol levels which can suppress progesterone production and shorten the luteal phase. Stress is one of the most underestimated factors in reproductive health and addressing it can make a real difference to your cycle.
How is luteal phase defect different from PMS?
Luteal phase defect and PMS both involve the second half of the cycle but they are different things. PMS refers to the symptoms — mood changes, bloating, breast tenderness — caused by hormonal shifts in the luteal phase. Luteal phase defect refers specifically to an insufficiency of progesterone or a shortened luteal phase that affects the uterine lining and fertility.
The Bottom Line
Luteal phase defect is a real and diagnosable condition that deserves more attention than it typically receives. If you have been struggling to conceive, experiencing early miscarriages, or noticing spotting before your period begins, it is absolutely worth raising with your doctor. A progesterone blood test and careful cycle tracking are straightforward first steps.
The most important thing you can do right now is start tracking your cycle in detail. Use our Free Ovulation Calculator to estimate your ovulation date and calculate your luteal phase length — and our Free Period Tracker to log your cycles over time. The data you collect over the next 2 to 3 months will give both you and your doctor a clear, evidence-based picture of what is happening in your cycle.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult your doctor, OB-GYN, or qualified healthcare provider for personal health decisions. Read our full Medical Disclaimer.